
The debate over the future of Britain’s healthcare system has been reignited by comments from Nigel Farage, who has suggested that an insurance-based model, closer to that used in the United States, could offer an alternative to the current structure of the National Health Service. While such proposals are often framed as pragmatic reform, they carry profound implications for patients, particularly those least able to absorb additional costs.
Farage’s argument rests in part on headline figures: £129 for a GP visit, £1,368 for an A&E visit, and nearly £72,000 for heart surgery. These numbers have been widely challenged, but their real significance lies in what they represent, a shift away from universal access toward a system where healthcare is mediated by ability to pay or insurance coverage. For many patients, that shift would fundamentally alter when, and even whether, they seek treatment.
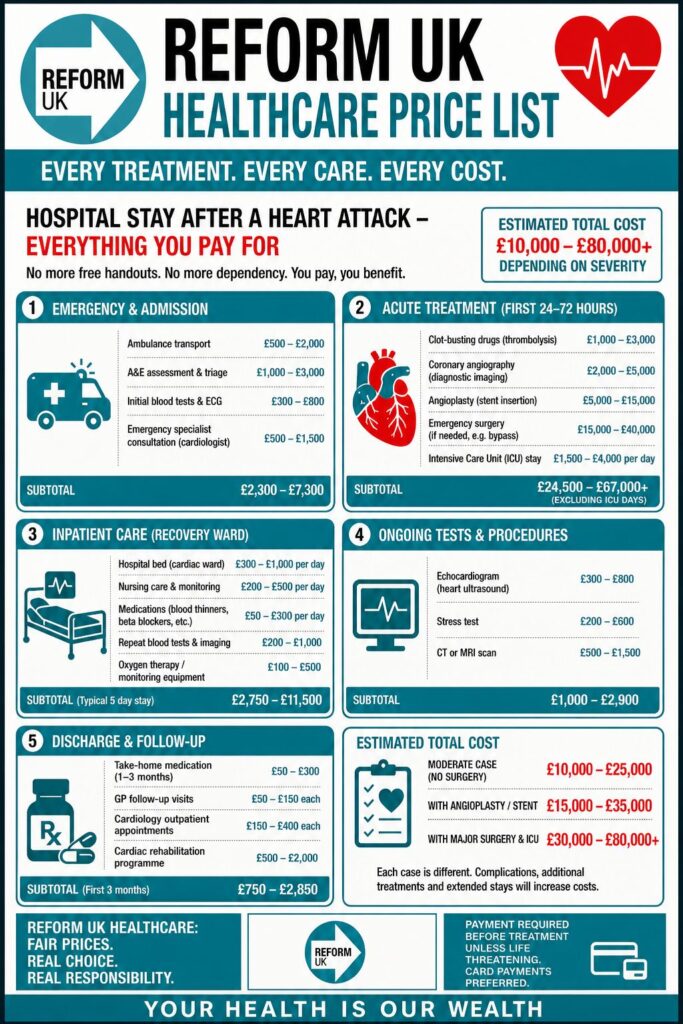
To understand the potential impact, it is useful to consider a hypothetical price list for common treatments if a US-style, insurance-based system were introduced in the UK. While exact costs vary widely in America, the following figures, converted and simplified, illustrate the scale of charges patients could face:
- GP appointment: £100–£200
- A&E visit (without admission): £1,000–£2,000
- Ambulance call-out: £500–£1,200
- Broken bone treatment: £2,500–£10,000
- Childbirth (standard delivery): £8,000–£15,000
- MRI scan: £1,000–£3,000
- Cancer treatment (annual): £50,000+
- Heart bypass surgery: £60,000–£100,000

Even in systems where insurance covers a portion of these costs, patients are often responsible for premiums, deductibles, and co-payments. The result is that healthcare decisions become financial calculations. Someone experiencing chest pain might hesitate before calling an ambulance, a parent might delay taking a child to A&E, and a patient with early symptoms might postpone a GP visit until their condition worsens. These delays can have serious, even fatal, consequences.
Supporters of the current NHS model argue that such scenarios are precisely what the system was designed to prevent. Under the Labour government, ministers have pointed to measurable improvements, including a reduction of 405,000 in waiting lists and faster ambulance response times for heart attack patients. While challenges remain, particularly around waiting times and workforce pressures, these are framed as problems to be solved within the existing framework, not by replacing it.
Critics of Farage’s position warn that an insurance-based system risks entrenching inequality. In the United States, those with comprehensive insurance often receive faster and more extensive care, while uninsured or underinsured individuals face significant barriers. Translating such a model to the UK could create a two-tier system, where access to timely treatment depends increasingly on income.
There is also the question of administrative overhead. Insurance-driven healthcare systems require complex billing infrastructure, claims processing, and dispute resolution mechanisms. This bureaucracy comes at a cost, one that is ultimately borne by patients through higher premiums or reduced coverage. By contrast, the NHS’s single-payer structure is comparatively efficient, directing a greater proportion of funding toward patient care.
Personal experiences further complicate the debate. While some patients cite long NHS waits as evidence of systemic failure, others emphasise the security of knowing that treatment will not result in financial hardship. For many, that peace of mind is not easily quantified but remains central to the value of the system.
The implications of Farage’s proposal are therefore not abstract. They would be felt in everyday decisions: whether to seek help, how quickly to act, and how much financial risk to accept. An insurance-based model does not simply change how healthcare is funded—it changes how it is experienced.
Ultimately, the question is one of priorities. A move toward a US-style system would represent a shift from healthcare as a universal right to healthcare as a conditional service. For patients across the UK, particularly those already vulnerable, that is not just a policy debate, it is a matter of access, security, and, in some cases, survival.




{kind=link}